
UDC 616.24 – 002.5 + 167 + 576.54 + 531.31/07-15-2013
DOI 10.24411/2658-3569-2020-10064
The starting factor in the onset and development of the TB – This «The cellular process of irreversible defatting»
Savchenko P.P., Orcid ID 0000-0001-5850-8307, J-2658-2015, Head, Professor of the International Research Center of Medicine and Substances «Intersuccess», Kiev, Ukraine, Sc.D, Ph.D, Academician of the Ukrainian Academy of Sciences, Honorary Professor of the University
«Lviv Stavropigion», u-spp@i.ua
Summary. The introduction of a principally new dynamic method in the history of phthisiology in the analysis of histological and cytological preparations, physical and chemical processes, the
sequence of the emergence and development of tuberculosis pathology, led to the discovery of «a radical starting factor in the onset and development of the tuberculous process in a living organism». This method fully identified with the principles of interdisciplinary approaches. For the first time, the dynamic method (discovered in physics in the mid-80s) was successfully tested in the 1990s into phthisiology and pulmonology; when we managed to remove the problematic and unclear issue of classical phthisiology: «On the mechanism of penetration of the mycobacterium from the surface of the organ into the focus, into the tissue». Namely, opened «The mechanism of penetration by means of her capture by an immune body and the subsequent movement by him in the living tissue, allowing an exit from anabiosis and reproduction of bacterium».
Key words: The dynamic interdisciplinary research method, The starting
factor in the onset and development of the TB (SFOD of TB), The cellular process of irreversible defatting (CPID), The osmiophilic lamellar bodies (OLB).
Data:
According to WHO statistics (1) Tuberculosis (TB) is one of the 10 leading causes of death in the world. According to 2015 data, 10.4 million people fell ill with tuberculosis, and 1.8 million people (including 0.4 million people with HIV) died from the disease; in 2015, 480,000 people worldwide developed multidrug-resistant tuberculosis (MDR-TB). About a third of the world’s population infected with a Koch bacillus. Why are more than 90% of carriers of tuberculosis mycobacteria healthy, and how does the immune system of these people fight the causative agent of the disease? – No final answer yet.
Of course, the existing contradictions and unanswered questions are the main obstacle in the fight against the disease. Mycobacterium confuses an outstanding intellectual and challenges medicine (2-4). Scientists note that the role of bacterial genomics, the coding mechanism of certain proteins of the host organism in the pathogenesis of tuberculosis is unclear.
Regarding the genomics of the organism, the carrier of the bacteria, the picture have the following: gamma-interferon (IFN-y) does not have protective properties against the tuberculosis bacterium; many echanisms, which explain cell-dеpendent immune defenses, including the involvement of regulatory T-cells in immune defenses, remain unclear. And the hypotheses put forward do not allow finding an effective solution. Scientists so far only express hope to understand the relationship of bacteria and the immune defense of the host organism with the use of new resources and technologies.
Humoral response of an organism observed, although for unknown reasons, he was not involved in protection against Mycobacterium (5). Scientists note that the interaction of mycobacteria with the body is incredibly complex. The bacteria found in the center of the granuloma, and inside the alveoli (outside the tissue). Marked accumulation of macrophages in the lung in the pathology. The role of many chemically active substances that are involved in phagocytosis in relation to mycobacteria remains unknown.
Scientists acknowledge that laboratories are unable to demonstrate mycobacterial damage in the presence of IFN-γ, TNF-α and a mixture of other stimulants. Many factors of immunity in the activation of lymphocytes remain unknown. Many components of the immune system are present but do not work with respect to infection; therefore, it is very difficult to identify the mechanisms involved in the immune system’s defense against infection.
This casts doubt on the standard mechanism (weakening of the immune defense) of the onset of tuberculosis disease. What obliges us to look for a new starting factor in the onset of tuberculosis (6).
No less important, calling into question the standard trigger mechanism, are surgical methods of treating tuberculosis. According to scientists, the immune system is unable to control the growth of bacteria, and surgical treatment together with antibiotic therapy provides the cure for 85-90%
of patients with severe forms (7).
There is no doubt that with the ineffectiveness of chemotherapy, for example, patients with cavernous and fibro-cavernous tuberculosis are subject to surgical intervention (8-12). In phthisiosurgical practice, there were frequent cases when lung resections were, carried out during the period of the process sharpening and, were not accompanied by severe postoperative complications and relapses, and in 60-80% of patients ended with a full therapeutic effect (13-16).
Surgery is perhaps the most complex process that weakens the immune system. There is a serious contradiction with the generally accepted triggering factor of tuberculosis, namely, a weakening of the immune system gives rise to the process, and during surgery for unknown reasons – recovery (17). It is very difficult to accept the fact, but on the other hand, it requires the search for a different starting factor, which has no contradictions.
Objective:
Conducting a study using a new interdisciplinary dynamic method of histological and cytological pathological material in order to identify the triggering factor for the onset and development of the tuberculous process in the host body.
Materials and Methods:
For the first time, we applied in phthisiology a new interdisciplinary dynamic method for the analysis of histological and cytological pathological tissue material after resection. The tragedy and complexity of tuberculosis is that it is difficult to answer the question – what is an early tuberculosis complex, based on histological and cytological material, when the drug allows you to observe the structure exclusively in a stationary state.
It was the new method eliminated this complexity. We carried out a comparative retrospective cross-assessment of our own and other material with basic histological and cytological materials (micrographs and descriptive parts), which were obtained in phthisiology from the 40s of the last century to the present day (18-26) with hypotheses that contradict the actual results, as well as the results of their own research from 1994 to 2010 (27-32).
The process of irreversible degreasing was previously put forward as a hypothesis, which was empirically confirmed in 2010, for example, for the first time in the sources of the Ministry of Health, the discovery was announced in 2004 (33).
In this study, the starting factor of the onset and development of the tuberculosis process experimentally confirmed in the dynamics of changes recorded in cytological and histological preparations.
The article is the final material on the topic «Specific and nonspecific lung diseases» regarding tuberculosis inflammation. Another material regarding the dynamics of pathological processes regarding non-specific diseases planned to publish in the near future.
Results:
Own micro-shooting and shooting from phthisiology materials, regarding the fundamental elements, coincide completely; no significant differences found.
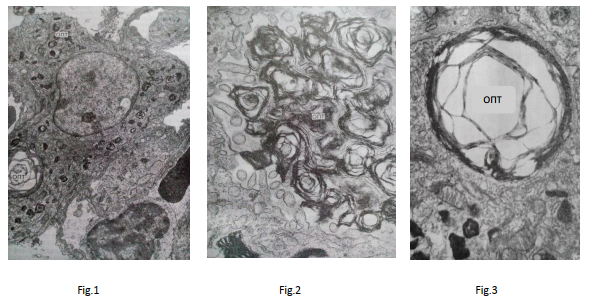
So, Fig. 1 shows the micrograph, magnification 9200, the formation of OLB in type 2 alveolocytes. In Fig. 2 – an increase of 30,000, the accumulation of optic conglomerates on the alveolar surface in the lung tissue adjacent to the granuloma. And in Fig. 3 – an increase of 15,300, the depleted-type OLB in the type 2 alveolocytes located near the tuberculous focus. Descriptive
materials in appearance are practically no different.
The following changes recorded which directly related to the new starting factor:
- the dynamics of the development of the tuberculosis process and the formation of pathological changes has a direction from healthy tissue to the center of tuberculosis education (tubercle, tuberculoma);
- phagocytic fragments of type 2 alveolocytes were found into the cytoplasm of the largest macrophages in front of the focal area, which confirms the activation of the immune system and the elimination of its own pathological cells;
- into the alveoli found: extracellularly located fat droplets; various stages of macrophage obesity are traced, which confirms the elimination of fatty substances by macrophages;
- disturbed ultrastructures of the OBD found: some osmiophilic bodies enlarged, vacuolated in the “pre-foci” area; lamel’s of others are separated by wide bright spaces; thinning of the lamel’s occurs, their stratification and destruction with a decrease in high osmiophilia;
- sometimes instead of OBD, a vacuole is formed with the remains of osmiophilous lamel’s in the pre-zone of the focus and in the focus;
damage to surfactant on the alveolar surface; - violation of the mechanisms for removal of spent surfactant from the alveoli;
- violation of the mechanisms of neurohumoral regulation of surface active properties of surfactant and other changes.
Conclusion:
The dynamic method allowed us to establish the following:
- From the zone of extra-tuberculous formation and as we approach the center of the focus, persistent changes in the decrease in the synthesis of surfactant in cellular structures, including the final ones, OLB, recorded. This process is characteristic of synthesis, in which there is a decrease due to the lack of starting materials for the synthesis of surfactant when they insufficiently supplied from the outside.
- In the pre-zone of the outbreak, type 2 alveolocytes, in which the OLB structures are thinned and stratified, do not absorb fatty elements, unlike type 2 alveolocytes, in which the OLB structures are preserved and which perform additional functions instead of pathological cells; revealed additional fat droplets, which corresponds to the mechanism of substitution function.
- Pathological type 2 alveolocytes, in which the structures destroyed, synthesize radical surfactant due to the lack of fatty compounds, which has a damaged structure and is difficult to remove from the surface of the alveoli.
Given the above, it is determined that in the zone of the pre-hearth there is a dynamic cellular process of irreversible defatting.
Thus, the new starting factor of the emergence of the tuberculosis process in dynamics is «the cellular process of irreversible defatting associated with impaired fat transfer for the synthesis of organic compounds»; and from the moment this process begins, the cell turns from
a healthy structure to a tuberculosis one and pathological synthesis of radical surfactant begins.
The prerequisites for the start of the cellular irreversible defatting process are the increased energy expenditure of fats in the body necessary for the synthesis of surfactant, and their (fats) short supply from the outside to the host body. When a tuberculous process occurs, metabolic disorders of other substances do not have a significant effect.
The discovery of the starting factor associated with impaired metabolism of fats, allows «for the first time» to explain the positive relationship of fats in pathophysiology and treatment of tuberculosis. This connection established earlier by various scientists, but remained unknown.
The discovery of this trigger factor allows us to remove the main contradictions in the classical theory in the future, solve the primary tasks of TB in prevention and treatment, and come close to the development of new drugs and methods of treating tuberculosis.
References
1. ВОЗ, Туберкулез, Информационный бюллетень Октябрь 2016 г.; электронный источник –
http://www.who.int/mediacentre/factsheets/fs104/ru/
2. Stefan H.E. Kaufmann, Stewart T. Cole, Valerie Mizrahi, Eric Rubin, and Carl Nathan, 2006
Mycobacterium tuberculosis and the host response, DOI: 10.1084/jem.20050842/ Published June 6,
2005, электронный источник – http://jem.rupress.org/content/201/11/1693
3. Divangahi, M., Mostowy, S., Coulombe, F., Kozak, R., Guillot, L., Veyrier, F., Kobayashi, K. S.,
Flavell, R. A., Gros, P., Behr, M. A. (2008). NOD2-Deficient Mice Have Impaired Resistance to
Mycobacterium tuberculosis Infection through Defective Innate and Adaptive Immunity. J. Immunol.
181: 7157-7165. http://www.jimmunol.org/cgi/content/abstract/181/10/7157
4. Kursar M., Koch M., Mittrucker H.-W., Nouailles G., Bonhagen K., Kamradt T., Kaufmann S. H. E.
(2007). Cutting Edge: Regulatory T Cells Prevent Efficient Clearance of Mycobacterium tuberculosis.
J. Immunol. 178: 2661-2665. электронный источник
– http://www.jimmunol.org/cgi/content/abstract/178/5/2661
5. Alamelu Raja, Immunology of tuberculosis; Department of Immunology, Tuberculosis Research
Centre (ICMR), Chennai, India; Received April 8, 2004; Review Article; Indian J Med Res 120,
October 2004, pp 213-232; электронный источник – http://www.icmr.nic.in/ijmr/2004/1002.pdf
6. Savchenko P ,International Medicine & Substance Research Center «Intersuccess», Phthisiology, Kiev,
«Debatable questions on problems of tuberculosis», Book of Abstract, 19th Conference of the
International Union Lang Disease, Africa Region, “Tuberculosis and Other Lung Disease: successes
and challenges”; Kigali Serena Hotel, 20 — 22 June 2013, (p.66).
7. Фещенко Ю.И., Ильницкий И.Г., Мельник В.М., Мельник В.П., Панасюк А.В., «Пульмонология
и фтизиатрия», Национальный учебник, стр. 82-83, 877.
8. Альба М.Н. Обоснование ранних оперативных вмешательств у вновь выявленных больных с
ограниченными формами туберкулёза: Автореферат к диссертации, к.м.н., М. 1997. 18 стр..
9. Амосов Н.М., Очерки торакальной хирургии, Государственное медицинское изд-во УССР,
Киев, 1958, 728 стр..
10. Волошин Я.М. Часткові резекції легень у вперше виявлених хворих деструктивним
туберкульозом. Автореферат к диссертации к.м.н., Київ, 1992, 18 стр..
11. Залескис Р. Роль хирургических методов в лечении туберкулеза, Проблемы туберкулеза, 2001,
№ 9, Стр. 3-5.
12. Перельман М.И., Наумов В.Н., Добкин В.Г. и др. Показания к хирургическому лечению больных
туберкулезом легких, Проблемы туберкулеза, 2002, № 2, стр. 51 – 55.
13.Репин Ю.М., Левашев Ю.Н., Елькин А.В. Показания к хирургическому лечению туберкулеза
легких, Научные труды и материалы конференции памяти М.М. Авербаха (к 75-летию со дня
рождения), М., 2000, стр. 229.
14. Гиллер Д.Б., Гиллер Б.М., Гиллер Г.В. и др., Хирургическое лечение больных остро
прогрессирующим туберкулезом легких, Проблемы туберкулеза и болезней легких, 2004, № 10,
стр. 23-26.
15. Борщевский В.В., Богомазова А.В., Гуревич Г.Л. и др., Ситуация по туберкулезу и внедрение
новых технологий организации противотуберкулезной помощи населению
Беларуси/Современные подходы к хирургическому лечению торакального и внелегочного
туберкулеза: Материалы республиканской научно-практической конференции (ноябрь 2002 г.),
Минск: КИН МВД Республики Беларусь, 2002, стр. 3-7.
16. Хоменко В.И., Мишин В.Ю., Чуканов В.И. и др., Диагностика, клиника и тактика лечения
остропрогрессирующих форм туберкулеза, Проблемы туберкулеза, 1999, № 1, стр. 22-26.
17. Савченко П.П., Керівник Міжнародного науково-дослідного центру медицини та речовини,
(Київ) «Дискусійні питання на проблему туберкульозу», НАУКОВО-ПРАКТИЧНА
КОНФЕРЕНЦІЯ «Актуальні проблеми профілактики, діагностики і лікування туберкульозу. До
150-річчя з дня народження академіка Ф. Г. Яновського», м. Київ, 17 червня 2010 р.
(http://www.ifp.kiev.ua/doc/news/temp/tubconf2010prog-1.pdf ), електрона версія докладу –
http://www.medlinks.ru/article.php?sid=41521 .
18. Авербах М.М., Гергерт В.Я, Литвинов В.И., Повышенная чувствительность замедленного
типа и легочный процесс, М., Медицина, 1974, стр.246.
19. Агапов Ю.Я., Бондарев И.М., Волкова Н.В., Активность легочного сурфактанта при
экспериментальном туберкулезе, Проблема туберкулеза, 1976, №6, стр. 73-77.
20. Бондарев М.М., Гулевская С.А., Немсадзе М.Н. и др., Морфология начальных этапов Lтрансформации микобактерий туберкулёза при сканирующей электронной микроскопии,
Проблемы туберкулеза, 1976, №12, стр. 55-61.
21. Ерохин В.В., Изучение легочной ткани в растровом электронном микроскопе, Архив
патологии, 1974, №1, стр.95-97.
22. Ерохин В.В., Молекулярные, субклеточные и клеточные механизмы патогенеза
туберкулезного воспаления легких, Саратовский научно-медицинский журнал, 2009, том 5, № 2,
стр. 267-269.
23. Ерохин В.В., Морфофункциональное состояние клеточных элементов туберкулезной
гранулемы, Архив патологии, 1978, №6 стр.37-44.
24. Ерохин В.В., Ультраструктурные и метаболические изменения легких при
экспериментальном туберкулезе, Проблемы туберкулеза, 1981, №4, стр. 61-64.
25. Нестеров Е.Н., Состояние сурфактанта и роль его изменений в патогенезе некоторых
заболеваний легких, Книга «Сурфактанты легкого в норме и патологии, под редакцией
Березовского В.А., Киев, 1983, стр. 91-97».
26. Пузик В.И., Сравнительная морфологическая оценка соединительно-тканных реакций в
исходе туберкулезных и нетуберкулезных заболеваний легких, Труды Центрального научноисследовательского института туберкулеза, 1973, т.19, стр.143-149.
27. Пузик В.И., Силов В.Ф., Ерохин В.В. и др., Гистохимические и электронно-микроскопические
исследования по возрастной физиологии, М., 1973, т.1, стр.61-62.
28. Савченко П.П., Альтернативный взгляд о природе туберкулеза, Труды ТОВ «Научнопроизводственной фирмы «Спектр, ЛТД», выпуск 2, 1995.
29. Савченко П.П., Механизм возникновения заболеваний, в том числе онкологических,
туберкулеза, сахарного диабета и СПИДА. Лечение заболеваний, Свидетельство о регистрации
авторских прав №6615 от 19.11.2002
30. Савченко П.П., Механизм возникновения заболеваний. Туберкулез, ISBN 966-502-209-1, РВК
«Деснянська правда», Чернигов, 2004 г., Свидетельство о регистрации авторских прав № 6951
от 17.01.2003 .
31. Савченко П.П., Савченко Л.Л., Философия туберкулеза, LAP LAMBERT Academic Publishing,
ISBN: 3659112941, ISBN-13(EAN): 9783659112942, 27.04.2012.
32. Гордиенко С., канд. мед. Наук, Альтернативный взгляд на туберкулез Савченко П.П., Газета
«2000», наука, 21.01.2005.
33. Савченко П.П., Нова гипотеза появи та розвитку туберкульозу, Медична Газета Мінздраву
України, № 50 (776), 2004.